Committed to Protecting Your Vision | Advanced Ophthalmic Care
Diabetic Retinopathy: The Hidden Danger in
Uncontrolled Diabetes
Are Your Patients Getting Their Annual Eye Exams?
Diabetes is widely recognized for its effects on the heart, kidneys, and nerves, but one of its most devastating & frequently overlooked complications strikes where you might least expect it: the eye. Diabetic Retinopathy is the leading cause of preventable blindness among working-age adults & in the vast majority of cases, timely detection can prevent irreversible vision loss.
What Is Diabetic Retinopathy?
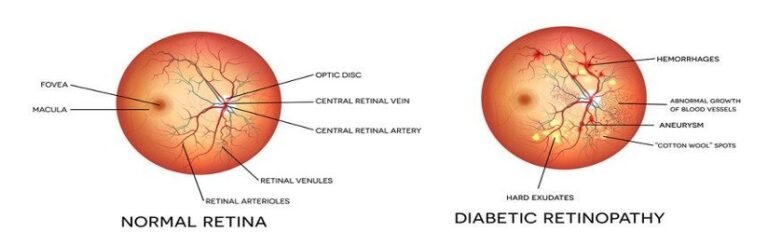
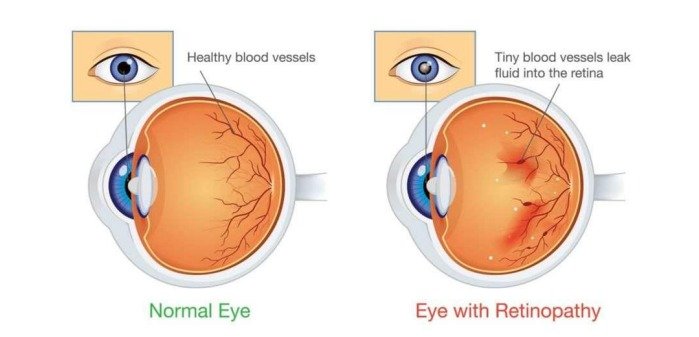
Diabetic Retinopathy (DR) is a microvascular complication of diabetes mellitus that damages the blood vessels supplying the retina the light-sensitive tissue at the back of the eye. Chronically elevated blood glucose levels cause these tiny vessels to weaken, leak, or grow abnormally, progressively impairing vision and, if left untreated, leading to permanent blindness.
How high blood sugar gradually damages the retinal blood vessels, leading to Diabetic Retinopathy
What makes DR particularly dangerous is its silent progression. In the early stages, most patients experience no symptoms whatsoever — no pain, no noticeable change in vision — even as significant retinal damage is quietly taking place.
Who Is at Risk?
Diabetic Retinopathy
Diabetes affects multiple systems — the eye is one of the earliest and most vulnerable organs impacted
Every person living with diabetes is at risk for diabetic retinopathy. The likelihood increases significantly with:
• Duration of diabetes: After 20 years, nearly all Type 1 and over 60% of Type 2 diabetic patients show some degree of retinopathy.
• Poor glycaemic control: High HbA1c levels accelerate retinal vessel damage
• Uncontrolled hypertension: High blood pressure compounds vascular injury in the retina.
• Elevated blood lipids (dyslipidaemia): Contributes to hard exudate formation and macular involvement.
• Pregnancy (gestational diabetes): Rapid hormonal changes can trigger or worsen retinopathy.
• Smoking: Accelerates microvascular degeneration throughout the body, including the retina.
• Nephropathy: Patients with diabetic kidney disease are at significantly higher risk
Stages of Diabetic Retinopathy
Diabetic retinopathy progresses through well-defined clinical stages. Early identification at any stage allows for effective intervention:
Mild NPDR
Small areas of balloon-like swelling
(microaneurysms) appear in retinal
vessels
Usually none
Moderate NPDR
Some blood vessels that nourish the
retina become blocked
Usually none or subtle blur
Severe NPDR
Large areas of blocked vessels; retina
signals the body to grow new blood
vessels
Mild blurring possible
Proliferative DR (PDR)
Fragile new abnormal blood vessels
grow — may bleed into vitreous; risk of
retinal detachment
Sudden vision loss, floaters, dark curtain
Diabetic Macular
Oedema
Fluid accumulation at the macula (centre
of vision) — can occur at any DR stage
Distorted or blurred central vision
By the time a patient notices vision changes, retinopathy may already be in an advanced, harder-totreat stage. This is precisely why routine screening even in the absence of symptoms is non-negotiable.
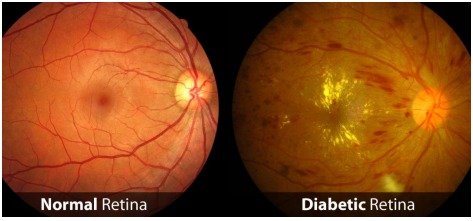
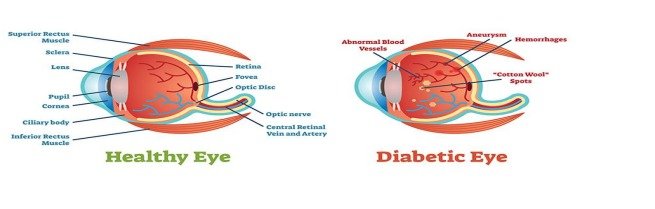
Normal healthy retina (left) vs. diabetic retina showing leaking vessels & damage (right)
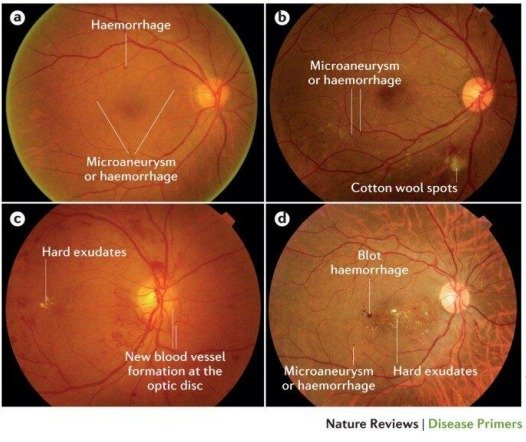
Clinical appearance of diabetic retinopathy — haemorrhages, exudates,& new vessel growth visible on
fundus exam.
A comprehensive dilated fundus examination by a qualified ophthalmologist remains the gold standard for
detecting diabetic retinopathy early. Yet, studies consistently show that a large proportion of diabetic patients
do not undergo annual eye screenings — often because they feel their vision is “fine.”
At Nair Super Specialty Eye Hospital, we strongly advocate that every diabetic patient — regardless of how
long they have had the condition or how well-controlled their sugar appears — must undergo a dilated eye
examination at least once a year.
Annual Eye Exam Checklist for Diabetic Patients:
Dilated fundus examination | Visual acuity testing | Intraocular pressure measurement | Optical
Coherence Tomography (OCT) for macular assessment | Fundus fluorescein angiography (when
indicated)
For patients with Type 1 Diabetes, screening should begin within 5 years of diagnosis. For Type 2 Diabetes,
screening should begin at the time of diagnosis — since many patients have had undetected diabetes for years
before it is formally identified.
A Message to Referring Physicians and General Practitioners
As the primary care physician or diabetologist managing a diabetic patient’s overall health, you play a pivotal role in
protecting their vision. We encourage you to:
1. Make ophthalmology referral a standard part of your diabetic care protocol — not an afterthought or a
reactive measure.
2. Document and track annual eye exam compliance for every diabetic patient in your panel.
3. Educate patients on the asymptomatic nature of early DR — “I can see fine” is not a reliable indicator
of retinal health.
4. Flag high-risk patients (poor HbA1c, hypertension, long diabetes duration) for more frequent screening —
every 6 months if needed.
5. Coordinate care closely — optimising systemic glycaemic and blood pressure control is equally critical
alongside eye care
Treatment Options: The Earlier, the Better
When detected early, diabetic retinopathy is highly manageable. The treatment approach depends on the stage:
• Observation and monitoring: Mild NPDR with good systemic control may only require close surveillance
and lifestyle optimisation.
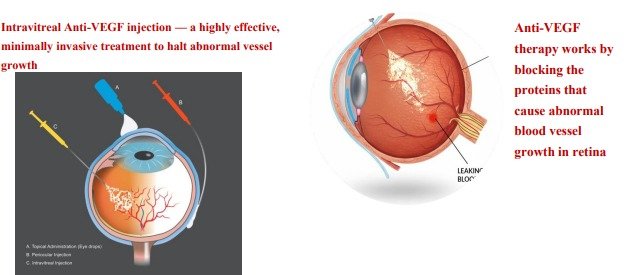
• Intravitreal Anti-VEGF Injections: First-line treatment for Diabetic Macular Oedema and proliferative
DR — highly effective in halting abnormal vessel growth and reducing macular swelling.
• Laser Photocoagulation: Pan-retinal photocoagulation (PRP) to seal leaking vessels and reduce the
stimulus for new abnormal vessel growth in severe NPDR and PDR.
The critical point: treatment is far more effective — and far less complex — when retinopathy is caught in its
early or moderate stages. Advanced-stage surgery carries greater risk and less predictable visual outcomes
Protecting Vision Through Systemic Control
Controlling blood sugar, blood pressure, & cholesterol is equally critical to protecting your retinal health
Eye care and diabetes management are inseparable. In parallel with ophthalmological treatment, patients must
be supported in achieving:
• Target HbA1c levels as advised by their endocrinologist or diabetologist (typically below 7% for most
patients)
• Blood pressure control — targeting less than 130/80 mmHg
• Lipid management — addressing dyslipidaemia with appropriate medications and diet
• Smoking cessation — an independent modifiable risk factor
• Regular physical activity and a diabetes-appropriate diet
